Bill de Bass joined the British Army as a Short Service Commissioned officer in 1967. He spent his first couple of years as a Regimental Medical Officer in 1st Regiment Royal Horse Artillery under the benign influence of (then) Lieutenant Colonel Ken Perkins (later Major General and Commander SAF from 1975-1977)
Looking to broaden his experience - and his horizons! - Bill sought a new role and relocated to Queen Alexandra’s Military Hospital at Millbank in 1969 for initial training in anaesthesia. This was followed by a posting to the British Military Hospital in Rinteln, Northern Germany - then the largest military hospital within the area controlled by the British Army of The Rhine.
One of only three anaesthetists there, he provided services for general surgery, a busy obstetric department and the various specialist departments.
In March 1972 he was detached to 55 Field Surgical Team in Salalah, formed specially to support operations in Dhofar. Bill cites this as a life-changing responsibility. His experiences in Dhofar - at a critical period and in the most basic, isolated conditions
"Now my theme is going to be 55 field surgical team in the spring and in the summer of 1972. What is a field surgical team? The field surgical team produces critical care as close as possible to the point of injury. And one of the things that it does is it then moves patients on to a base hospital. And the base hospital that I started with was BMH Rintel.
My story starts in an upper corridor in BMH Rintel, which was a 250 bedded hospital in BAOR. I had been a 27 year old anaesthetist there for a number of years and the hospital covered surgery, eyes and obstetrics. I was making my way along the top gallery near the physiotherapy department when I came across a Battery Sergeant Major who had been in my original regiment in the Army, 1st RHA. I listened very patiently as Battery Sergeant Major McDonough told me how he had been injured somewhere in the south of Oman. To be truthful, I did not pay too much attention, but took most of it on board and wished him a speedy recovery.
Back in theatre, I met with my anaesthetic operating theatre technician for the day, Private Peter Canning, RAMC, who with an amused grin announced that the Commanding Officer wanted to see me. Interview with our coffee, sir? Red light, speeding.
The Chief Clark ushered me into the CEO's office and he greeted me and said, sit down, Bill. Would you prefer tea or coffee or a biscuit? The interview was not going the way Private Peter Canning, our EMC, wanted it to go.
You are to be detached to an FST in RAF Solana in Dhofar. I don't suppose you know where that is.
Well, no, I don't actually know. I didn't actually know where that was until I came across Battery Sergeant Major McDonough. And I said to the COO, rather bravel,y that I did know where it was. And he said, typical smart aleck anaesthetist who is always several steps ahead of everybody else. I confessed that I didn't know anything about field surgical teams but could I visit one please to familiarise myself. His response was that there are no field surgical teams in the British Army other than those that are actually working.
So the cup of coffee that had been offered to me in BMH Rintown was offered to other people. It was offered to people in East Alan, Catterick, Tidworth, Cambridge, at Aldershot, and also at the Warwick Hospital.
I left a very unhappy Colonel Roger and I returned to the operating theatre. Colonel Roger had just lost one of his three anaesthetists and they were going to be away for six months. This would slash his operating capacity by more than 33% and severely cramp the hospital's surgical throughput. At that time, the 180,000 soldiers in the British Army were treated in several hospitals, 13 to be precise, which was really very short. There was going to be nobody to replace me whilst I was away.
The ever inquisitive canning that I am going to be detached with at Salalah, doubted that he even knew where that was.
South of Oman, sir, he said surprisingly. There is a guerrilla war going on there. Lots of shooting, SAS involved. I wouldn't go there, sir, if I was...
Smart alec operating theatre technician who knows everything one step ahead of everybody else. Well, Canning, I said, the CEO said that as you and I get on so well together, you can come and hold my hand.
Those of us that would be unceremoniously strapped, detached from our comfortable postings in BAOR, and in the UK, were invited to the assemble at the Skeletal Two Fields Hospital in Mitchet. We were jabbed with various vaccinations, immunoglobulin 3 doses. We were issued with OGs, given some weapon training, and began to get to know each other.
Our new best friends, RAF Air Movements, shipped us as live cargo to RAF Salalah, where they offloaded us into a dusty shack on the edge of the airfield. We had one day of handover from the departing team.
Remarkably, the first person I anaesthetized was the outgoing anaesthetist. He had got a bad back and he, the consultant, trusted me to put him to sleep so he could be loaded onto the plane.

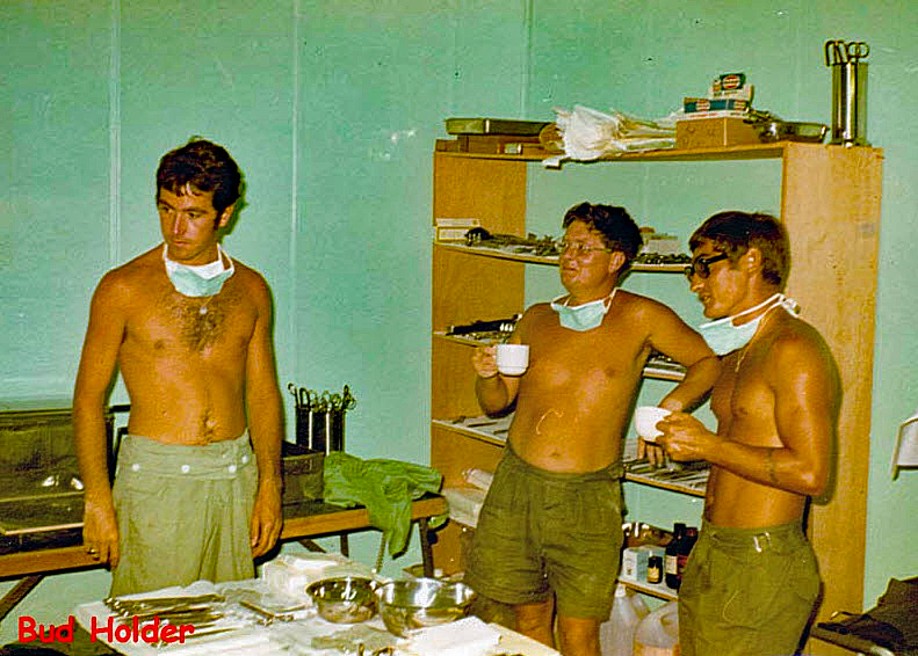
We then decided we would have to have a team photograph. And we started, obviously, we've got to have a commanding officer. We started with Joe Johnston, who was an Irishman from Tidworth, and he was a very experienced and charismatic surgeon, backed up by me as the anaesthetist who was really woefully inexperienced. The junior surgeon was Captain Nick Chetty, who had been with the Scots Guards. We then had the Mafia, the four operating theatre technicians, led by Jerry Farrell, who is over on the right there. That's Jerry Farrell, and then Bud Holder, and also Pete Starling. And, of course, Private Peter Canning, R.E.M.C.
The operating theatre technicians were certainly the backbone of the field surgical team. The nursing element was led by somebody called McPargin and he had two SRNs with him as well, Sergeant Lynn and Sergeant Mack. We had an X-ray technician, Sergeant Roger Hicks, who worked with very, very primitive apparatus and did an absolutely wonderful job. The last person who was on the technical side was Dave Barrow, who looked after the path lab and also the blood supplies. The last person, Tony Powell, was the Clark who kept everything together.
Everybody has to take a photograph, and the man who took this photograph was a man called Chief Tech Spice. He was our interface between us and the RAF. After all, the medical centre was on his signature.
Who were we going to look after? We were going to look after Batt. That's the real reason that we were there. We were there to provide them with surgical care. But there were other people who we looked after as well. Obviously, those people we looked after. But there were one or two others who we also took care of. We took care of some sailors from British merchant ships. We even took care of a gibbon that belonged to one of the SAF officers.
But the elephant in the room was the Adu. We did look after the Adu as well. And the matter with the Adu was that they hadn't got any care up on the Jabbal, so they might come to us.
This is quite a crude slide. And it shows the people who were injured after the battle at Merbat. The 2 SAF people at the top, Walid Kamis in the middle, who was the second. And then further along we get Adu, get Adu, Adu and Adu. So they were looked after as well, which was no bad thing. They were operated on in strict order. We didn't put them forward, we didn't put them back, but they were there in clinical need. They had some miserable equipment on the Jebbel. They had this crude first aid kit, which wouldn't have done any help to anybody. If any of them were badly surgically injured, they would be put on a camel and go to Health or to Al-Gaida and then on to Aden.
Our patients came on helicopters, Jet Ranger or Huey. The Jet Ranger wasn't really very useful because if with one patient on board, they couldn't really give them any medical attention. But with the Huey, you could have two people on board and a couple of medical assistants and that worked very well.
Adam Cowley, was an American surgeon. He had been a military man, and he'd come up with the idea that if you get somebody to surgery within an hour, they've got a much better opportunity of surviving. And he pushed this forwards. These are the people who came back from Meurer, and they came perhaps one hour at least by helicopter. So they were actually outside the golden hour. There, one of the fuzzy people is Neville Baker. The next person to him is Takavizi, walking characteristically, even though he was badly injured. And the next person is Joe Johnston. They were put into a tent for triage. They were put on the floor. There were quite a lot of them, so we were a bit short of space. There were 23 of them who arrived on the helicopters quite quickly.
The helicopters, of course, hadn't been able to go into Murbat early because Neville Baker was shot at quite badly as he was going in. And he went back to Tacker, put the helicopter down, saw what the damage was, and then when it was safe to go back to Murbat,
He went back and then brought them along to us.
Henry V, Act 4, Act 5, Scene 1, Sergeant Williams, the fictional Sergeant Williams. What he said was, blood is the argument. And as it was 550 years ago, blood still is the argument. We didn't have a blood bank. We had a rusty fridge.
Then the patients, of course, were moved on to the operating theatre. This is your 1972 high-grade operating theatre. It's a five F section F.S.T. Inside, it was equally primitive. These are the two operating theatre technicians, myself in the back, the one on the left, Private Peter Canning Army.
Happily, the Royal Engineers Troop came to our aid, and they put up the Twyneham Hut for us. The left hand side of it was resuscitation. The right hand side of it was a 16 foot by 16 foot operating theatre. The operating theatre technicians thought it was wonderful. The one who's missing there is Private Peter Katie.
What do you do to begin with when somebody is injured? Well, the first thing to do is to assess what's going on with them. You assess when they were wounded. You assess what their wounds were. You then perhaps look at them and see what is right or wrong with them. Are you going to give them a pre-med? Most of them didn't have a pre-med. Also you didn't ask all the questions you might have asked. You don't ask somebody from that, whether he's sensitive to Lubin. He's likely to give you an answer that takes no account of rank.
Then your object is to get some allen into them. It's our key to anesthetic in your job is to get them into their brains and put them to sleep.
You start off by putting them to sleep with Thiopentone. Thiopentone or Pentethal is used and it puts them to sleep in about 45 seconds. They're already dosed up with atropine, which dries them up and stabilizes their hearts. An 8 millimeter tube is brought down into their lungs. And then they are paralyzed with the same thing that Russian tourists used in Salisbury.
Once they're asleep, you then have to keep them asleep for a long time, and you have to paralyze them for a long time. This man, Thomas Waterton, was the squire of Walton Hall near Wakefield, and he had been in Guyana looking after his family farms. And he got interested in the people who used to hunt with poison-tipped arrows. And what he did was bring some of the arrows home, these little darts. He brought them home to Walton Hall, and then he scratched the shoulder of a donkey, and the donkey stopped breathing, which was bad news because the donkey was effectively dead. He took some bellows, he pumped the donkey's lungs, and eventually the donkey recovered. He actually lived for about 30 years. That's exactly what we did in Salalah. We put a tube down somebody's throat and inflate their lungs. And the tube has to go deep down into the trachea. Now, that's a deep, dark hole. And I quote after this, what they're all like Charles Bowden, the good Catholic and Lucy in these that say, they say when they're putting, intubating somebody, and putting a tube down in the name of the Father and of the Son and into the hole it goes.
There is a difficult airway society. And that is for people who, for one reason or another, are difficult to intubate. It might be because you're overweight, it might be because you've got a short picnic, it might be because you drink a lot of sherry. My first difficult airway was in this man. You may be familiar to some of you.
And he went to sleep quite successfully, actually. My trainer, Colonel Voller, he said, anaesthetising, he said, I'll stay in the operating theatre office reading the newspaper and you just get on with it. Some intubations can be difficult as the face is damaged. It's difficult to get a tube down. This lady, we call the little old lady from the left, she had, from the west, she had been injured somewhere near South Vate about three days earlier. And we brought her into the FST and then on to the hospital and spent three or four operations, reconstructing her face.
This man had an injury high up in his neck and we simply couldn't get a tube down. And I made a tracheostomy and the tube went down into his lungs. Incidentally, he was added.
The machine that I used in order to transfer the anesthetic into patients consisted of a mask, some valves, some bellows, and you might think it was oxygen. But there was very little oxygen there. That was all the oxygen we had. We could only scrounge oxygen from airworks, and we were very, very grateful for the oxygen that we gave us.
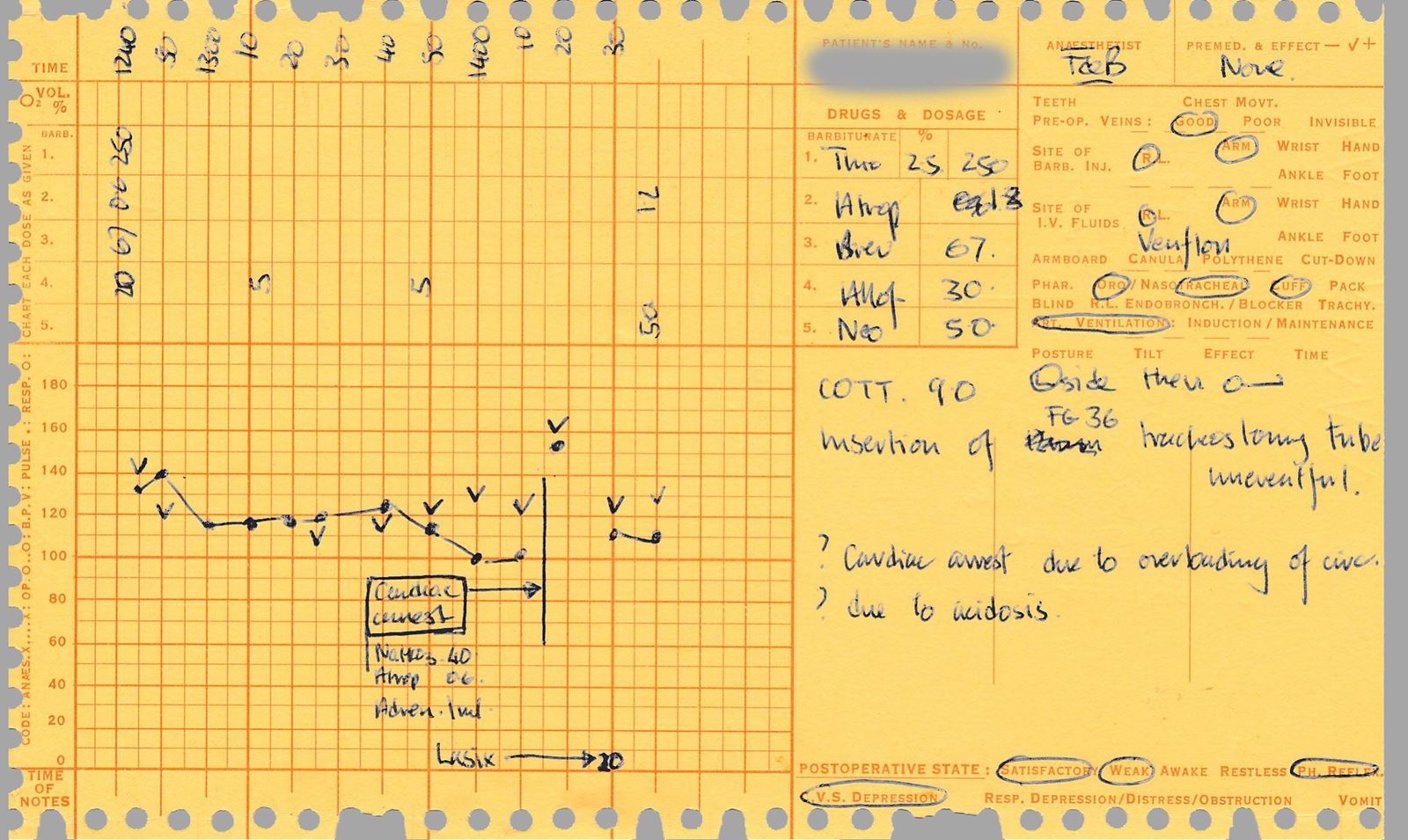
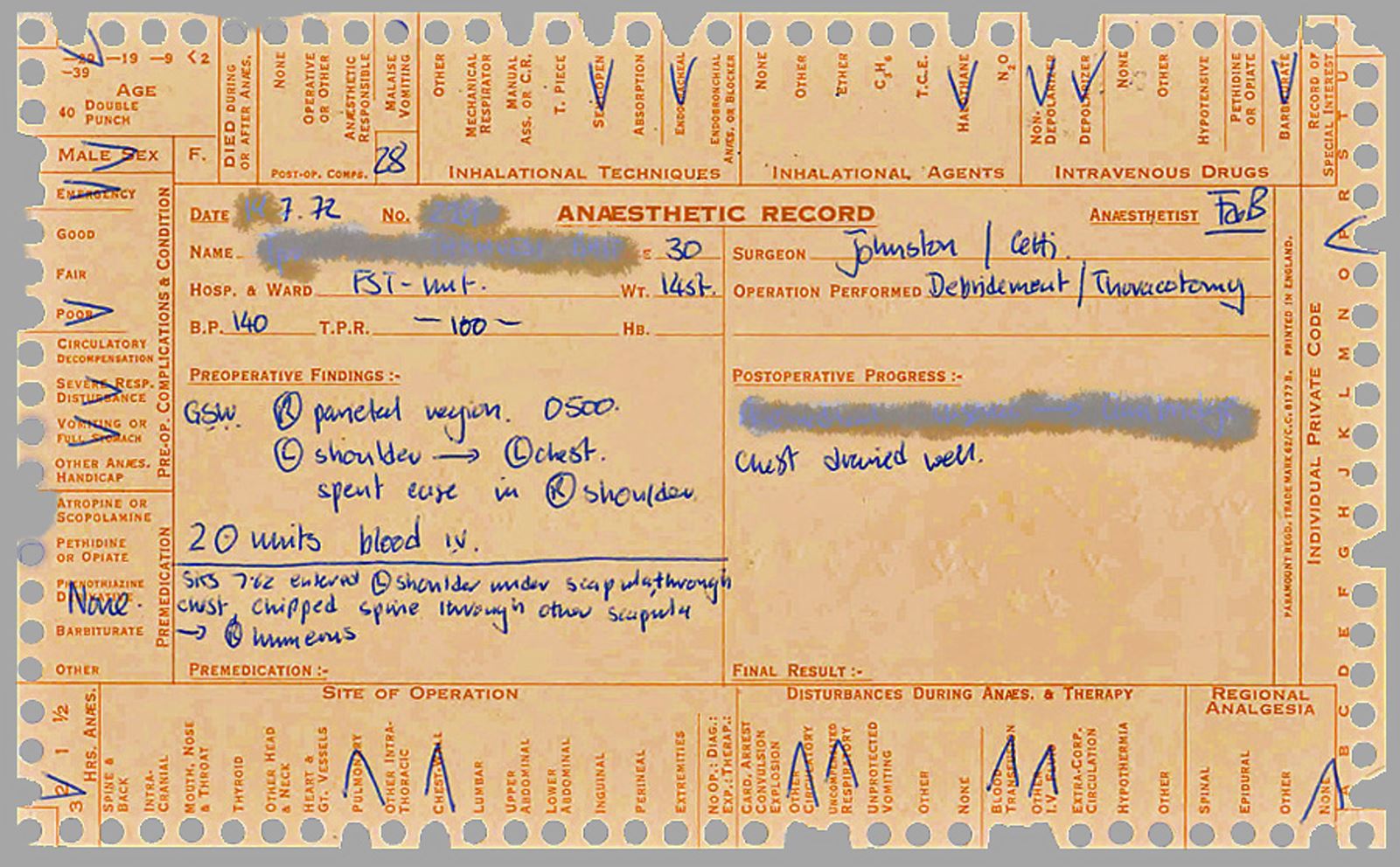
Back to our patient cards and what happened was I made the records and there when something had happened, for example up there you can see that his state was poor and he tipped it out and you could sort them out by putting a knitting needle through the whole lot of them, shaking it and then when the ones that you wanted. His injury that I recorded started was at 5:00 in the morning. You can see that we first operated on him at 12.40, so he was well outside the golden hour, which is really quite important. There's a lot of other information on here. He had a cardiac arrest halfway through, put him on his back to start with, left hand side, and then on, sorry, left hand side, and then on his back. I think it was probably something to do with a treatment that caused the cardiac arrest.
I now go through to some selected injuries, injuries from an AK-47. There's a huge amount of energy in an AK-47 bullet. The bullet there is coming through that block of gelatin, just to illustrate that.
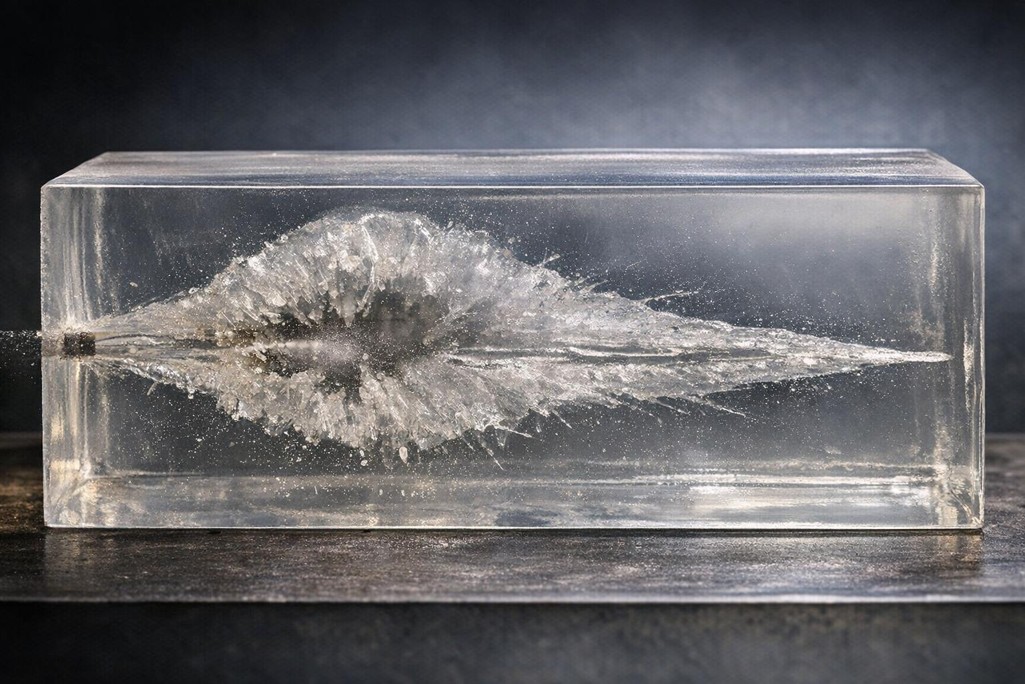
There's an entry wound. Now the entry wound in that child's leg looks really quite small. It is quite small, but you can see there where the femur, the big bone has been shattered by that and there are all lots of little fragments there. The exit wound is horrendous and massive.
Tiny little one to start with on this side, hugely on the outside. Once you start taking it to pieces on the clean it up, you can see all those bits that are black and dead. All those have to be removed or the man will get gangrene. This is the man who didn't get gangrene. His leg was put in a splint. He was strung up into the beam there and he was absolutely terrified. He thought we were going to hang him.
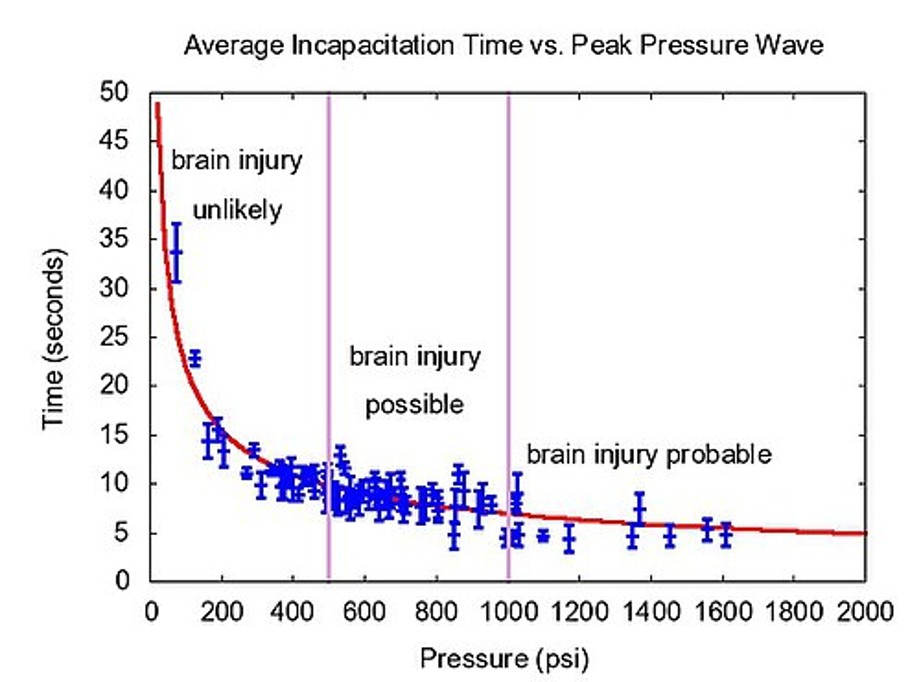
Now these, there are two, I can see three bullet wounds here. One there, one there, entrance wound. That one went all the way over there to his left shoulder. But also he had a bullet wound in his skull. It didn't go through his skull, but it just traversed his skull. And what that did was put a big shockwave through his skull, which was equally damaging. You can see here damage. If you've got 0 to 400 pounds per square inch, brain injury unlikely. 1600 pounds, brain injury significantly likely.
Now, one of the people died was Tom Tobin. He was shot in the jaw, and being shot in the jaw put a shock through his skull, and that caused brain damage.
Traumatic blast injury can be amalgamated with traumatic brain injury.
This man, Barry O'Driscoll, I was at school with and I played rugby with him. He was obsessed with minor head injuries. He thought that everybody who had a minor head injury, it was cumulative and it caused injury to them.
This man, I also played rugby with, familiar to many of you. He played rugby as well, and consistently injured himself, and I had to put him right rather than downgrade him medically.
The military explosive is entirely different. The pressure is absolutely huge and very abrupt and causes damage which spreads throughout the body.
The PNN mine, with about 249 grams of explosive, causes rather more damage than is needed to injure or to incapacitate somebody.
This man has been injured by a PNM mine where it's taken off his left leg. And what it has done is it's taken it off just below the knee.
He gets a nice stamp at the end of it after Joe Johnston has worked on him. And then Air Works, very generously, would glue 3 planks together. They'd bore a hole in the middle, put a bit of plastic pile on the bottom, and then we had a good false leg.
The bigger minds, the TM-46, were nasty things. And the only way to protect against them was with the man-bladed vehicles.
Furiously enough, if somebody was driving this vehicle and the line went off under the right front hand wheel, the person in the left hand side might not be injured at all. This man was, he was badly injured by an AM 46. You can see there where a huge line of skull was knocked out. You can see there where we made a hole in his skull to see if there was any blood inside and there wasn't. He died instantly and I think was buried in the cemetery in Salalah. There are short-term effects of blast injury, and they are easy to recognize, like losing a leg. There are also long-term effects, which are less obvious. There are effects to the cardiovascular system, emotional effects, metabolic effects, and some unusual ones like heterotrophic calcification. When you have a blast injury, it damages the tendons, the muscles and the nerves, and the muscles and the nerves may get calcified. This can be very painful and may require surgery to move it.
The Imperial College of London, the Royal British Legion, has spent a lot of money funding a blast centre and with research into blast, and the military still continues to support them with in kind, but I don't think they do it with money.
Fragment injury is another thing. Mortars can give on significantly large fragments, and what they may do is hit a critical point. This particular Batt operative was mortared down in a root in the early part of May, and that mortar fragment transected his spinal cord and killed him very quickly.
The RCL was another thing which caused nasty big fragments, and the RCL that landed on the edge of the officer's mess, put 13 people onto our operating table in the next few hours.
One of them was a senior pilot, and you can see there where the round went through his leg. But more specifically, you can look at the lower part of the leg. If I just move that on, you can see how pale it is. Just move the leg slightly onwards, And it cuts off the arteries, and that causes huge problems.
Smaller fragments could causeapparently very little damage. You can see there's a peppery there in the back of this chap's leg.
Lots of little fragments in there that are very difficult to find and take out. They've got to be taken out because they will cause gangrene. It's heroic surgery. You can see how much has to be exposed, how much of the dead stuff has to be removed. But that's a very, very tedious job for the surgeon.
Another chap with slightly older injuries to the leg, and you can see You have to dissect a lot out, Hydrogen peroxide helps it cleanses wounds wonderfully.
How did we evacuate people? Well, first of all, they went into the Rainford Ward, which was a twine and hut, and they were put in beds, or they were put.
On the floor, then they were taken by ambulance. Mash was our ambulance that had been purloined for us by bat and driven down in the Gulf. The patients then went on to or to the Royal Salala Hospital if there were civilians. As the three people in the stages of recovery, you can see that I was quite busy.
English people were evacuated to the UK. Sometimes it was successful, sometimes it wasn't successful.
Sergeant Morse, who was injured in 1971, he had 22 pints of blood in a six-hour operation but the transit in the C130 back to Bahrain, he died, unfortunately.
We also worked in Salalah Royal Infirmary. We went allowed RAF patrol, so we had to go to the back of the palace where a blonde lady from Taylor Woodrow provided us with petrol. The hospital was really quite primitive and the entrance to the hospital was something that wasn't really very inviting.
The ladies outpatient was very, very smelling of frankincense.
We could operate on some things, but in order to come out successfully, we would have to have good post-operative care. This Duvali, we really wasn't worth operating on him. He'd had this for years and years and years since birth. And to operate when he wasn't being disadvantaged by was perfectly reasonable.
This man had been cauterized to try and help his eggs, but it didn't do any good, and he died as you might expect.
There were, although the worst of the worst separating, there was a women's ward, there was a children's ward, there was a men's ward. Also, there were opportunities for teaching. Joe and Nick took greater advantage of that. The operating theatre was a tile operating theatre, and we brought our own anaesthetic machine because they didn't have one. Our weapons, were looking at the window sill and the rest of us got along with it further down.
This woman, you might think at first glance, was pregnant. She wasn't pregnant. She got something called leiomyoma, and Joe removed that. You can see the tumor here, you can see her uterus here, and her ovaries here. Extraordinary as an orthopedic surgeon like Joe who does his hand to this.
This lady had a huge one, which took Joe 3 hours to remove. She invited us down to a meal on the beach.
It's a question of manning the equipment or equipping the man, and what we care about is that we had very poor equipment supply and Ludishol didn't do us very well. We needed equipment that was good. We needed equipment that was effective. We really could have done with oxygen in order to treat the blast injuries. We really could have done with something other than an x-ray machine that worked on more than just a three-bit plug.
We would have loved to have something like a diaphragm machine costing now only 1000 pounds, which would slash operating times in 1/2. The 40 hours we spent operating after could have been dropped down to 20 hours.
Equip the man. Well, the theatre technicians and the other ranks were extremely well equipped with their training. Very well equipped indeed. They had naturally accepted qualifications and they used them. If we go to the officers, the officers are a different kettle of fish. The senior officer, the CEO, Joe Johnston, was a particularly good surgeon. He was particularly experienced and he was absolutely excellent. As a second man down, myself, the anaesthetist,
I was inexperienced and quite frankly out of my depth. I'd only been doing the job for about four years and my predecessor had been a consultant and I should have been of a higher rank. It shouldn't have been me.
One thing that I might like to say is that having done all that we did there, we did quite a lot of work with the Omanis in the hospital. We sent things back to the UK for histopathological analysis and we did quite a lot of training. It was a start really of an Anglo Omani cooperation, which I think goes on to this day."
Q+A:
What did you do about rehabilitation? Did you have any rehabilitation services after?
No. No, we passed that on. We pushed it on to people in El Gwerth and any rehabilitation for people who were British people, they were evacuated back to the UK. But there wasn't anything set up then at that time.
It must take an incredible sort of mindset to be operating in an environment like that with such a level of natural life and death in your hand. How do you get into a headspace that enables you to operate effectively and how do you translate that perhaps outside of your researching?
How can you, how do you cope with it? I suppose when somebody appears in front of you and they've got serious injuries, you don't think about it, you don't get on with it. That's how you're trained, particularly if you're an anaesthetist who's only called upon when there's a problem. When there's a problem in the hospital, they almost always say call the anaesthetist. And also the surgeon, Joe, who had been a trauma surgeon, if he saw somebody who was particularly badly injured, he just got on with it. He didn't think about it. One of the things that we did, rather than wait until somebody was fit enough for surgery, we just went straight in and did it. You're going to have to operate on them sometime. And how did that help us in the future? I suppose it influenced the way in which we worked in the future in our professional lives.
I remember once being called for whatever 400 miles away to go to the airport at sea to give some blood because I was blood O negative. How on earth do you literally anyone with O negative in the north was told to report to the airport. How did you cope with the daily supplies of blood, which you must have needed?
The daily supply of blood was Dave Barrow going around RF Salalah and taking taking blood from people. He was quiet down the front of your shirt. What does your dog tag stay? I'll have some of that.
What did you do next?
What did I do next? What is the doctor? Oh, I left the RAMC. I stopped being an anaesthetist. I did some obstetrics and for that next 25 years I was not good. I was a GP in Norfolk.